Elite Recovery Protocols - Exposed
1 - INTRODUCTION
I would like to pull back the wool on advanced recovery protocols used in elite training and clinical circles and make them accessible to everyone. These approaches need to move from behind the shadows to becoming the standard of care in injury treatment and post-surgical interventions. It’s going to take people like myself taking a stand on this topic, raising the flag around the massive amount of science and proven results so that everyone can have access to these treatments. It’s not a discussion of performance enhancement but of tissue regeneration and reducing exposure to greater injuries, reducing health care cost and related recovery related costs and lost productivity. The contents of this document involve more than just recovery from injury—they hold the potential to significantly contribute to increased quality of life and reduction of pain.
The recovery protocol I’ll be detailing here is one I have developed over the last 15 years while working with practitioners, researchers, biochemists, and related scientists and experimenters, not to mention elite athletes. Up to this point, much of this information has only made its way into circulation via the leaders in the fields with whom I’ve worked. You may recognize some components of this document as commonly used protocols. The level of depth and methodologies covered will surprise and even the most well-versed people on these topics and is far from just a just documentation, or regurgitation, of many of these protocols floating around the performance field.
What I have put together for you is the most comprehensive and integrated approach to these protocols you will find published anywhere at this time.
To provide an example of results that can be seen using these approaches, I reached out to a recent athlete I consulted, and he agreed to allow me to share. Understand this is a ‘typical result’. Travis Rogers’ experience was after a bilateral quad rupture after surgery in which the muscles were attached back to their origin on both legs. His initial rehab started in his wheelchair. With this program, he was able to regain his ability to walk and progress all the way to a 700lb deadlift in 12 weeks! Travis followed every component of this approach with substituting e-stim for the shockwave.

My lifting career is littered with “phenomenal’ recovery stories which are documented online. One such example involves a grade 2 tear of my quad. I went from being unable to complete even a bodyweight squat at the onset of this injury to just weeks later showing up at the Arnold Sports Festival and executing a 915 lb squat, a 600 lb bent over row for a double, and an 875lb deadlift all in under 5 minutes—fully recovered. I have helped numerous athletes who have suffered grade 2 quad tears like this--barely able walk and unable to even perform a partial bodyweight squat--to recovering and being at competition level within 3-4 weeks.
The intention of this piece is primarily an outline of the peptide and supplement protocols. But the overall process scope of the recovery process cannot be disregarded as it is not just “magic biochemistry’” to the rescue. For this reason, I will also do a cursory review of neurological signaling, movement, and fascial, manipulation approaches. Its important to understand the entire process and how these things work in concert and layer on top each other.
Recovery CANNOT be looked at through a structural healing lens only. But due to the depths of these topics, I will only be linking to appropriate sources that will provide further education on these subjects with methodologies aligned with the overarching approach I have employed.
The goal of this piece is to:
Display the framework of the approach
Detail the specific measured protocols
Provide links for education or sourcing
Citations are provided on the key biochemical areas.
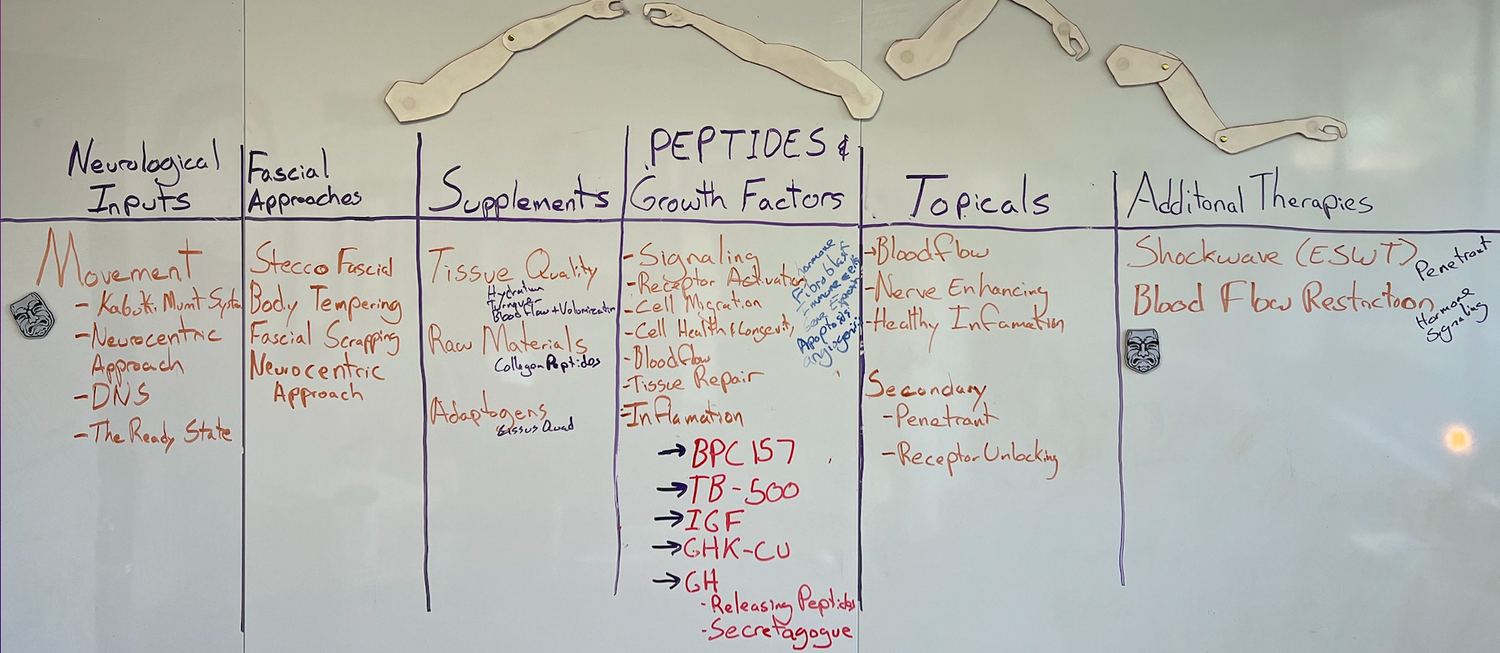
2 - MOVEMENT AND FASCIAL APPROACHES - NEUROLOGICAL INPUTS
The body prioritizes the health of nerve tissue over muscle and bone tissue. Often, muscles will tighten around an unrecognized, injured nerve in an attempt to splint and protect that irritated nerve. This protective muscle tension creates unbalanced movement around joints. Failure to understand this relationship in the training environment will often result in nagging muscle and joint injury. Recognizing and removing this neural irritation often removes the unbalanced muscle tension, reduces injury risk, and greatly (and quickly) improves performance. Removal of neural irritation may sometimes be achieved through movement alone and sometimes with manual therapy, as both enhance blood flow to the involved tissues and the mechanical interface of the nerve with the tissues around it. However, the magic is in using both movement and manual therapy in concert with one another. The best example of this 1-2 punch out there is the clinical protocols contained in the NeuroCentric Approach® (NCA).
The body will always protect nerves over tissue. If the body is mechanically compromised, this is when we are more likely to tear or strain a muscle or tendon. It is important to understand that the extra contractile effort engaged to protect neurology creates tension post-injury, limiting range of motion in a protective manner. This very protective measure, however, inhibits healing, as movement itself is healing in part due to its promotion of increased circulation and nutrients to the injured area. Facilitating good quality movement will begin to shut down the protective mechanism and allow you start expressing movement and loading capacity sooner. which will result in an increased healing process.
Some of these measures are best facilitated in a movement-based approach while in certain cases, a fascial-based approach may be used. Often, these two methodologies are employed in concert with one another. The best example of the utilization of a neurological lens to guide these choices in a clinical context can be found in the NeuroCentric Approach.
There are some notable other methodologies, educators, and practitioners that work off this same philosophy and lens with to view and guide approach. But as with some other areas of this document, I do not want to take on the responsibility to maintain and ‘approve” a database of approaches. In my extensive work in the field and with groups my confidence and results I have seen with NCA bar none. But at same time I do not want to be exclusionary as I am agnostic about who is behind an approach, it’s all about the overarching philosophy. The same can be said for all remaining references in this section below.
Once the shift begins to move from clinical to loading, or what we call ‘return to play’, the education and training models around which Kabuki Education is centered are a perfect fit. Kabuki Education’s methodologies were developed in concert with the same agnostic principal-based philosophies. I would be remiss if I didn’t mention that Kabuki Strength’s equipment facilitates proper loading strategies and neurological inputs.
If you do not have the aforementioned resources available, you may be able to find a local clinician trained in DNS (Dynamic Neuromuscular Stabilization), which forms part of the foundation of the broader systems referenced above. Dr. Kelly Starrett’s The Ready State is another agnostic system closely aligned with the principal-based subject of this document.
When it comes to fascial-based protocols I prefer tools I can use myself in conjunction with movement. I find this combination to be far superior to passive modalities. Kabuki Strength makes some incredibly unique Instrument Assisted Soft Tissue (IASTM) tools. Many of them were developed with Body Tempering Pioneer Donnie Thompson. Fascial Scraping can be done with the MyoRök, which is an incredible implement designed for this purpose. The MyoRök might be the only ‘mountable’ tool on the market, and its design, mountable on the ShouldeRok or a barbell, makes it an effective tool for self-use. For passive modalities, I endorse Stecco Fascial’s protocols.
3- SUPPLEMENTATION
Do not skip forward or you will be kicking yourself later! I know, I know, everyone wants to get to the grey area topics but you WILL NOT take full advantage of those rarely-discussed topics if you miss some key ideas here! I organized this document in a very specific manner in order to that reflects how each of its sections integrate and layer with one another.
I did keep the supplement list very short as you can really go down a rabbit hole on that front. Here, I just hit on the supplements that cover significant breadth.
Tissue Quality
The amplification method through improving tissue quality. I will get to exactly what I mean here shortly.
If you want to get the most out of your peptides, TRT, training, movement or soft tissue work as mentioned above, attention must be paid to supplementation that works in support of tissue quality. Supplementation can be used to stimulate blood flow to the muscle as well as keeping the tissue “full” of glucose stores. In the bodybuilding world this is known as a pump but can be facilitated in a 24/7 manner with the correct supplementation. The value in this is the improved cellular hydrated with the water bound to the glucose in the muscle belly. In turn the improved hydration and bloodflow transports more nutrients to the muscle and allows for byproducts and waste to be effectively cleared.
The tissue is more likely to respond to load and contraction in this state with improved tone. It is less likely to incur strains, tears, and cramps and certainly better adept at significantly enhancing recovery. This is what I mean by tissue quality. Enhancing tissue quality in this manner is an amplifier. It not only amplifies training, it amplifies everything you do--from good training, diet, or even peptides, TRT (as I cover in this video), PED’s and yes your direct soft tissue work as well.
The supplementation protocols involve Nitric Oxide supplied via a couple different pathways. Extensive citations regarding this are provided at the end of this document. It is also important to note this is accomplished with daily dosage filling the NO and NOS pathway alongside Lactate, as these supplements operate in a chronic vs acute fashion and need to develop a saturation level which is around 18-21 days. And of course, taken at the clinically effective dosages as noted in the cited research.
Unfortunately, there were no products on the market that met these needs without being loaded with stimulants as a preworkout. Entirely messing the chronic loading approach noted in the research. Seeing this gap is when I we brought VasoBlitz to market as the flagship product when Build Fast Formula was initially founded. Vasoblitz works to optimize blood flow through a variety of potent pathways, and as such, VasoBlitz contributes to the effectiveness of recovery protocols along with active training sessions.
I’m serious… tap your heels and say VasoBlitz, VasoBlitz, VasoBlitz 🤪🧬. 2 scoops a day every day. Before training… or bedroom training for that matter 😈, or anytime on off days.
Since this is a product that I’ve decided to be involved with because I am so passionate about the results, I have provided a couple pages of surrounding NO, NOS, and Lactate at the end of this document. All further citations will be identified appropriately within the text and included in the citations list.
Raw Materials
It is important to understand that in some cases you need physical stimulus, not just the raw materials supplements provide, to get the most out of your supplement protocol. For example, if you take calcium but don’t load your body, the body has no stimulus telling it to do the cellular work that will increase bone density--the same works the other way around. Movement and related work discussed in the first section creates this stimulus, and a fresh injury leaves raw receptors ready to receive. Save this thought for later and revisit it in the peptide section 😉
If you are dealing with any joint or connective tissue issues or engaging in extreme training/peaking (my period spent squatting 800 pounds daily is a good example of this intensity level and frequency), I recommend 40-60g a day of Collagen Peptides. This dosage is based on recovery state, not a general protocol. If an issue is muscular only AND I have a high level of collagen in my diet, I may drop that dosage significantly or entirely. There are few other ingredients needed to maximize the effectiveness of Collagen Peptides, so to keep it simple I recommend Vital Proteins as it includes all of those ingredients—not to mention the fact that Vital Proteins is an incredibly effective product in its own right. Post surgery protocol:
Collagen Peptides 40-60g/day
Vitamin C – 1g (enhances absorption of Collagen, increase over whats in Vital Proteins)
Zinc – 60mg (plays roll in Collagen synthesis)
Hyaluronic Acid – 100mg (included in Vital Proteins Brand)
Because of the general knowledge on this supplement, I’ve only added a couple citations on its impact to inflammation and bone turnover [1] and joint recovery from exercise [2].
Adaptogen
An adaptogen enhances the body’s ability to respond to stress. There are many types of these products on the market, and I utilize a number of them for my general health, both physical and mental. But when it comes to recovery from a major injury, Cissus quadrangularis is phenomenal. It increases wound healing, reduces inflammation and cortisol; but where it really shines is in relation to joint health, connective tissue support, and recovery from bone fractures [1]. I didn’t pull any studies on Cissus quadrangularis for this document, but I do remember seeing studies showing fracture healing increases around 30%-50%[2]Cissus quadrangularis also has a large positive impact on collagen type. Beware that it does have noticeable impact on pain perception [3] which may sound like a good thing, but it’s something you definitely need to be aware of as pain perception is a key indicator guiding your rehabilitation and healing process.
Controls inflammation: Excessive inflammation can turn out to be more aggravating and results in dilating blood vessels. This is known as hyperaemia and may leads to pain, swelling, and heat around the injured site. Hadjod evokes myeloperoxidase that yields cytotoxic acid (HOCI), cytokines and neutrophils, helping to reduce inflammation. Hence, Cissus quadrangularis supplement reduces the swelling and pain associated with bone, tendon, and ligament damage.
Lessen joint pain: According to a research study, individuals suffering from chronic joint pain, when advised to use Cissus Quadrangularis, showed about 31% decrease in pain. Another study claims Cissus Quadrangularis is used to decrease pain associated with mandibular fractures as well.
Lower healing time and speedy recovery Studies claim that Cissus Quadrangularis supplement lessens healing time of the bone by 53% and its uses include upsurge in bone mineralization. Another study discloses hadjod’s ability to preserve and retain bones strength and thickness.
A great product that contains Cisssus and several other complementary products (Palmitoylethanolamide, Andrographolide, Boswellin®, UC-II® along with Bioperine® for absorption) is Leviathan Joint Support. Code (no kickbacks) for 10% off: Duffin
4- PEPTIDES RESEARCH & PROTOCOLS
Oh yeah, this is the section you’ve been waiting for--or maybe have been afraid of 🤪. I’ll start off by dropping the base protocols with some initial details, then move on to the research summaries. The first 3 items have become quite prevalent in protocols within anti-aging clinics these last few years. I’ve spent over a decade revising and refining these approaches on myself and others.
There are also some oral approaches to some of the protocol that I will detail as well. Both Tb-500 and BPC-157 can be delivered systematical via oral delivery if bound to an arginate salt. And one of the ways of increasing IGF levels can be done with an oral peptide as well. I have seen spray versions of these products but have not done the research to vouch for their efficacy. But do know that for GI issues the BPC arginate salt is the way to go.
Protocol Summary
TB-500: 500mcg per day before bed (Subcutaneous/SubQ or Intramuscular/IM Injections)
BPC-157: 350-500mcg Twice daily AM/PM (IM in site)
IGF1-LR3 or* or GH Releasing Peptides
iGF at 50mcg twice daily (split in two different muscle belly sections leading into site so 25mcg each -3 weeks on 3 off)
*A combo of CJC-1295 (no DAC) / Ipamoralin 200/100mcg up to 500/250mcg 2x a day
GHK-CU 1mg 1-2x daily (causes Fair but post injection pain 10-40min)
That last one is likely one you have not heard about outside of cosmetic use such as topicals for skin and hair. I have had significant success with adding this to the protocols and it will ramp up the impact of the peptides preceding it in this list to another level. Beware of the post injection pain as it can be fairly intense in some areas, but usually quite tolerable in most. I’ll drop some more detail below on why this is so effective. If you have connective tissue-specific issues I would make this a much higher priority in your protocol design.
Due to the massive amount of available information on IGF, GH, and GH Releasing peptides available these two areas’ I did not provide citations and left that for the other areas.
You will note that all my links are to Limitless Nootropics. Be aware that there are some shady companies in the peptide industry due to regulation or lack thereof. You want to do your diligence and make sure you have a trustworthy source, and just like the clinical area I do not want to take on the responsibility for maintaining qualified vendor list. I have chosen to link Limitless Nootropics due to the quality and availability of compounds. I have also worked with them to get a 15% discount for my audience.
Use Code Duff15 for 15% off at Limitless Nootropics.
Get proper syringes and bacteriostatic water hereBPC157 and TB-500 Summary
I’m covering these two in concert as they have some similar properties and are nearly always combined together due to the synergistic nature. Key characteristics include:
Both peptides include strong anti-inflammatory properties [11][12][10]
Both repair damage to muscle, heart, skin, ligaments, and organs while BPC also works on Bone.[13][14][15][16]
BPC-157 also increases vasodilatation much like VasoBlitz but also increases formation of new blood vessels (angiogenesis) [6][7][8][9][10][17][18][1]
TB-500 also provides pain relief and also boosts immunity[20][21]
You can see how this mix of qualities can deliver impressive results for all types of healing and how its garnered the name “wolverine stack’. Strong anti-inflammatory properties, direct tissue healing, and improved bloodflow is a power packed combo.
Actin and Cell Migration
The protein Actin is what the movement of fibroblast which regulate extracellular matrix production rely heavy on. This also includes the cell walls of the immune system. Both BP7-157 and TB-500 work at the level of the gene in regulation of the of actin and increasing its production[1].
BP7-157 and TB-500 work together increasing actin and through that the migration of fibroblast and immune system cells to the injury sites.[2]
Fibroblast Growth Hormone Receptors
Again BP7-157 and TB-500 work synergistically but in regards to increasing the growth hormone receptors on the fibroblasts.[3]
➡️ This is where the use of the IGF discussed early becomes important. These cells now have a longer lifespan due to the increased growth hormone receptors along with plenty of actin for that longer lifespan.
We now have the signaling setup. What would be the last thing that we need to add??
Raw Materials!
➡️ Now the supplementation of the Collagen Peptides comes into play and we have everything set in place for maximal tissue regeneration.
⏫⏫⏫⏫⏫⏫⏫
Can you now see how these items have bend dubbed the Wolverine Stack?
Deeper Dive into all things IGF and GH
IGF-1 LR3
With IGF its always a great move to up-regulate the receptors with some brief movement or loading of the area.
IGF LR3 is more effective if you have major trauma when administered post-surgery, but it requires a bit more handling and knowledge. LR3 needs to be reconstituted with .05% (NOT .5%) acetic acid solution versus Bacteriostatic Water that is more readily available. Because it is reconstituted in an acid, after drawing yoru dose into your needle for administration you should backload another 15+ units of Bacteriostatic Water into the syringe to reduce the PH. The acetic acid is needed while in the vial so that it doesn’t degrade but adding water into the syringe right before administration will be better than injecting it as an acid. This will also help it disperse into the tissue further.
LR3 down-regulates the receptors very quick due to how powerful it is, thus the short periods of time running it. And even then, you most likely will no longer see an effect after a few cycles if the injury isn’t significantly acute trauma. That said, LR3 is powerful so you don’t usually need that many cycles 🤪. I do have a variety of other depending on the severity of the injury as well as where it falls in the acute vs chronic spectrum based on experience with myself and athletes over last 15 years. This is based soley on experience learning how how heighted the trauma, and thus receptors, are and the frequecncy and duration of injections that will keep working. Some examples:
25mcg x 2 day Every Other Day EOD for 4-6 weeks
25mcg Every 3rd Day E3D for 12+ weeks
It should be noted that the 25mcg dose reduces spillover, which is not desirable as the greatest concentration of IGF receptors are in the gut.
I can provide guidance/coaching on IGF or any of these protocols if needed.
Another way to elevate IGF levels is to increase Growth Hormone directly.
Growth Hormone
You might be surprised to find that I don’t have a direct recommendation for GH in this approach. I have not found any NEED for it with the above methods and the IGF delivers the fraction of GH responsible for the healing properties without the side effects. Personally, I have not found GH to be worth the money for what it delivers compared to GH releasing peptides that appear to have significantly less long-term side effects.
Little bit of a tangent but GH blunts output of the pituitary among things like negatively impacting blood glucose levels while peptides increase natural release with very little sides.
If you are in fact using GH therapy I would recommend continuing to do so as you don’t want to reduce output during recovery. A dosage of 1-2 IU a day 5 days a week would be adequate.
Growth Hormone Releasing Peptides
My preference is to go the route of adding GNRH peptides / GH Secretagogue. There are several different products that fall in this category but reviewing all of them and the numerous approaches’ would be an article in itself. For this application let’s keep it simple and use a combination that’s typically available in a solution together, CJC-1295 (without DAC) is also known as Mod GRF 129 along with Ipamorelin. This can be administered 1-3x a day with higher frequencies allowing the total dose to be higher due to the short half-life. I find twice a day to be adequate for recovery needs.
For those wanting a non-injectable to combine the Oral approach with BPC157 and TB500 bound to an arginate salt a highly effect oral GH boosting secretagogue is MK-677 to increasing IGF levels. There are a couple downfalls with MK-677 that make me not provide any dosage guidelines and add some hesitation. First is the massive increase in appetite, which may not be of concern, the second being its negative impact on blood sugar levels.
It should also be noted that you can stimulate additional GH release via BFR training which we will dive into specifically later in this article.
GHK-CU Summary
GHK-Cu is rarely if ever discussed or included in healing protocols which is unfortunate due to the profound impact it has. I hope to change this by providing some exposure to this little-known compound outside the cosmetic arena for skin and hair. This copper peptide provides the following key properties for wound healing:
Suppresses chronic inflammation (different pathways than BPC and TB500)
Increases collagen production
Massive for the proteins in the protective skin barrier
Provides the signaling for tissue remodeling!
Increased bloodflow
Pain reduction
Now I want to state that GHK-Cu can be quite fairly effective for pain, but can cause a fair bit of post injection pain in the 10-40min range. In some areas this can be quite intense and others barely noticeable. In rat models, GHK-Cu had a dose-dependent effect on pain-induced behavior. The pain killing effect is from increased levels of the natural painkiller L-lysinel12 creating these analgesic affects [1]. Another analgesic Amino acid L-arginine is also increased[2]. This type of pain reduction is highly preferential to NSAIDs.
I had noted increased volumeisation of tissue injected with GHK which makes since with the L-arginine improving vasodilation just like BPC-157 but also found research confirming the formation of new blood vessels as well [3].
The bullet point on improved signaling for remodeling is also quite interesting. GHK draws fibroblasts, immune cells, and endothelial cells to the site of injury and appears to coordinate their activity in repairing the damage. While stimulating the synthesis and breakdown of collagen, glycosaminoglycans, and other extracellular matrix components like proteoglycans and chondroitin sulfate [4]
It is probably worth noting that GHK-Cu contains properties. Since this only relates to open wounds or skin repair, I’ll skip detailing this out and dropping citations. Although anecdotally I have seen one person inject it into an abscess in concert with antibiotics and it did appear to speed the recovery process. But that’s hardly a data point to reference and I only share for entertainment.
While its properties make it pretty potent for increasing healing of connective tissue, let it be understood that it works nearly as well for all soft tissue. I have noted that it will bring some additional fluids to the area during its use but have not seen any research supporting the vasodilation effects noted with BPC. And unlike BPC-157, it does NOT appear to have any affect on bone.
GHK-Cu CNS and Brain Function
One area I find absolutely fascinating regarding GHK-Cu is the Neurological component. The neurological component of healing is often overlooked. It actually shows it can improve angiogenesis within the nervous system! Yes, that’s right, reducing inflammation within the CNS as well as increasing growth! Evidence suggest that it can help create a state of health even in a dysfunctional system by resetting pathological gene expression[5].
Many degenerative diseases such as Alzheimer’s are poorly understood but it is found that GHK-Cu in the brain does decline with age. So, the question becomes is the degenerative diseases of the brain a result of this decline or caused by it? A number of scientists do believe that with lower GHK-Cu levels the nervous system tissue is less able to fight off issues and any resulting dysregulation may be what actually leads to neurodegeneration. This is just theoretical at this point although some evidence does support it--some of which is from rat studies. One study suggested GHK-Cu may help prevent normal cell death and protect the brain or even improving neurological deficits and swelling during brain bleeds or strokes[6].
I find these topics quite interesting and not unrelated to the discussion here.
TOPICALS
Time to pimp some CBD creams 🤪. Just kidding, but at same time, there is some validity to the application of CBD products to some healing protocols. CBD can certainly be useful in unlocking receptors. combine that with a good penetrant and now you have the ability to drive those peptides you just injected deeper into the cracks and crevices you didn’t reach, as well as prime the receptors.
What we want is a topical the improves nerve signaling and limits the “threat” signaling and related retraction of the nerve endings and related inhibition and tightening of muscles around it. This was covered in the first section of this document. The goal of the topical is to facilitate the same measures.
Topicals can be great at increasing blood flow to the area as well, once again facilitating what is happing with the vasodilation supplements and peptides enhancing recovery.
The last component is promoting positive inflammation and bringing down non-productive inflammation with the use of products like curcumin and other botanicals for example.
If you want some research on this one all I got is… well fuck me… haha not my area of expertise but I’ve seen the effects with great products and know the biochemist who formulate them. So I’ll link them below. But you will note my clients use them like Travis Rogers and they can tell the difference once including them in the protocol. I have talked extensively with the formulators about what I’m doing and developed this approach of layering the topical with peptide application in concert with them.
Heat
These last few discussion points are why we want to add heat as well. I thought dropping this in the topical section would make the most sense. Heat over ice is going to be the primary approach. I often get asked why not cycle between the two. Simply put, you have halved your time for apply heat which is what you want 🤪
Nerve Cream
I recommend Proze Nerve Cream that was developed by Biochemist I know while he was working with Greg Roskopf the founder of MAT/Muscle Activation Technique. It works amazing as a stand-alone product but using Proze post-peptide injection absolutely improves the efficacy of the peptide.
I do have one other topical I use that is not on the market yet but the above biochemist is working with another innovative doctor I know to develop it. I hope to add this here as well.
Enhanced Nerve Function
Enhanced blood flow
Promotes healthy inflammation
Penetrant to drive products into tissue
Unlock receptors
You can use code Duffin25 when purchasing Proze Nerve Cream to save some cash. As with most of the links or codes provided in this document, I don’t get any kickback. I have these codes because each product or service is something I personally use, believe in, and promote.
ADDITIONAL THERAPY
Shockwave Therapy
I have found shockwave therapy beneficial on its own as a treatment modality. But I have discovered some unique applications outside of its FDA approved listings:
Extracorporeal shock wave therapy (ESWT) is a noninvasive treatment that involves delivery of shock waves to injured soft tissue to reduce pain and promote healing. According to Jonathan T. Finnoff, D.O., medical director for Mayo Clinic Sports Medicine at Mayo Clinic Square in Minneapolis, ESWT is a viable option to consider for many patients who present with chronic tendinopathy that hasn't responded to more-conservative treatments. Often difficult to treat, chronic tendinopathy is characterized by localized pain and pathological changes to a tendon. The condition affects athletes and nonathletes alike.
Shockwave therapy has a consistently demonstrated effect on relieving excess tissue tone. It is highly effective at doing PRIOR to the IASTM soft tissue work discussed at the beginning of the document. This saves significant time in getting to deeper work on areas holding a lot of tension. You’ll net better results when these modalities are done in this sequence in both scope and longevity.
Professional Shockwave Similar to mine
Why isn’t shockwave therapy at the beginning of this article as you stated this document is organized with intent and layered?
Oh yeah… Did I mention shockwave therapy drives products even deeper? It does--it drives topicals and injectables deeper into the tissue and disperses them within the tissue. Yeah, that….
Peptide ➡️ Topical ➡️ Shockwave ➡️ Soft Tissue work OR Movement work
Blood Flow Restriction
So much for the quick article I was going bang out before work in the morning 🤪. Can I just keep this section brief and reference all the articles, video’s, and podcasts I’ve done on this subject?
BFR is incredible for its ability to induce change with low loads which is of critical importance during recovery. BFR works to increase blood flow and increase GH release.
Blood Flow Restriction Rehabilitation (BFR) is a paradigm-shifting intervention for the rehabilitation professional with over 160 peer-reviewed articles in the scientific literature. By applying a tourniquet briefly and intermittently to an exercising limb you can induce significant and substantial strength, hypertrophy and endurance changes while using a very light load. Link to research on the linked product page.
Light exercise with BRF Bands produces a quick and easy muscle fatigue.
A fatigued muscle sends a signal to the brain that a metabolic change has occurred. You feel the muscle burn; your brain takes action.
The Pituitary Gland releases a rush of Growth Hormone (GH). GH is the most powerful hormone in the body.
The body responds to this GH release by secreting other hormones that create positive changes in muscle after exercise.
This GH hormone surge also creates a whole host of other health benefits in your body. (Anti-aging, cardiovascular, bone, and many other benefits)
Because you have used light weights or have done light exercise, the recovery time will be reduced.
Think about how this works in concert with everything discussed up to this point. Think about the synergistic effect with using a product that facilitates bloodflow, pump, and recovery like VasoBlitz.
I should note that the Kabuki Kratos Flywheel enhances the results of BFR training with its constant time under tension. And it has a lot of research on the rehabilitation side in regards to Tendon Stiffness. This tool was used by Travis Rogers in his recovery, and you will notice Dr Kelly Starrett. (the Supple Leopard) of The Ready State used it in his recent knee replacement post-surgery stating “the Kratos Flywheel needs to be a central modality in rehab practices, particularly in post-surgical interventions.”
Addendum – Origin Story
As I was adding the examples to the introduction, I realized that one of the moments that these protocols really started to gel is documented quite well. Back in 2010 I detached the sternal and clavicula head of my left pec. I documented the entire recovery on my youtube link about how this works. At the time I implemented the IGF protocol post-surgery that I was well versed in for years at this point. I was doing the supplement protocol with only cissus and collagen at the time and was looking for a practitioner to do the fascial scrapping technique that was quite rare at the time.
During that search I met Doctor Philip Snell who was the first one in our state to do that technique, but he was off exploring new more innovative stuff by that time. And what he introduced to me during the that period was what ended up gelling into our Kabuki Movement Systems approach and his NeuroCentric approach many years later.
It should be noted that in these very early days only using portions of the approach at that time I made a crazy recovery. At 6 months post-surgery I was bench pressing 405 for 20 reps over 3 sets at 9 months post-surgery I set the 4th highest all-time total in the 198lb class in powerlifting. The standard for this surgery was to be released to light training at 6 months, full training at 12 months, and was told I would never be as strong as I was before the surgery.
Research Citations
Collagen Peptides
[1] https://pubmed.ncbi.nlm.nih.gov/30783776/
[2] https://pubmed.ncbi.nlm.nih.gov/34491424/
Cissus Quadrangularis
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4784127/
[3]https://www.tandfonline.com/doi/abs/10.3810/psm.2013.09.2021
BPC-157 and TB500
[1] C.-H. Chang, W.-C. Tsai, M.-S. Lin, Y.-H. Hsu, and J.-H. S. Pang, "The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration," J. Appl. Physiol., vol. 110, no. 3, pp. 774-780, Oct. [Physiology.org]
[2] J. Kim and Y. Jung, "Potential Role of Thymosin Beta 4 in Liver Fibrosis," Int. J. Mol. Sci., vol. 16, no. 5, pp. 10624- 10635, May 2015. [NCBI]
[3] C.-H. Chang, W.-C. Tsai, Y.-H. Hsu, and J.-H. S. Pang, "Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts," Mol. Basel Switz., vol. 19, no. 11, pp. 19066-19077, Nov. 2014. [NCBI]
[4] Song, Ran & Choi, Hyun & Yang, Hyung-In & Yoo, Myung & Park, Yong-Beom & Kim, Kyoung. (2012). Association between serum thymosin ß4 levels of rheumatoid arthritis patients and disease activity and response to therapy. Clinical rheumatology. 31. 1253-8. 10.1007/s10067-012-2011-7. [Research Gate]
[5] Philp, D., et al. "Thymosin 34 Promotes Angiogenesis, Wound Healing, and Hair Follicle Development." Mechanisms of Aging and Development, vol. 125, no. 2, Feb. 2004, pp. 113-115, 10.1016/.mad.2003.11.005. (PubMed]
[6] T. Huang et al., "Body protective compound-157 enhances alkali-burn wound healing in vivo and promotes proliferation, migration, and angiogenesis in vitro," Drug Des. Devel. Ther., vol. 9, pp. 2485-2499, 2015. [PubMed]
[7], pp. 774-780, Oct. 2010. [PubMed] [8] Y.-L. Hu et al., "FAK and paxillin dynamics at focal adhesions in the protrusions of migrating cells," Sci. Rep. vol. 4, p. 6024, Aug. 2014. [Nature.com]
[9] P. Sikiric et al., "Novel Cytoprotective Mediator, Stable Gastric Pentadecapeptide BPC 157. Vascular Recruitment and Gastrointestinal Tract Healing," Curr. Pharm. Des., vol. 24, no. 18, pp. 1990-2001, 2018. [PubMed]
[10] - Vitam Horm. 2016;102:251-75. doi: 10.1016/bs.vh.2016.04.005. Epub 2016 May 24. Thymosin ß4 Promotes Dermal Healing. Kleinman HK], Sosne G2
[11] F. Amic et al., "Bypassing major venous occlusion and duodenal lesions in rats, and therapy with the stable gastric pentadecapeptide BC 157, L-NAME and L-arginine," World J. Gastroenterol., vol. 24, no. 47, pp. 5366-5378, Dec. 2018. [PubMed]
[12] K. Skrlec et al., "Engineering recombinant Lactococcus lactis as a delivery vehicle for BPC-157 peptide with antioxidant activities," Appl. Microbiol. Biotechnol., vol. 102, no. 23, pp. 0103-10117, Dec. 2018. [PubMed]
[13] S. Seiwerth et al., "BPC 157 and Standard Angiogenic Growth Factors. Gastrointestinal Tract Healing, Lessons from Tendon, Ligament, Muscle and Bone Healing," Curr. Pharm. Des., vol. 24, no. 18, pp. 1972-1989, 2018. [PubMed]
[14] - Expert Opin Biol Ther. 2015;15 Suppl 1:5139- 45.do:10.1517/14712598.2015. 1011617. Epub 2015 Jun 22. Advances in the basic and clinical applications of thymosin B4. Goldstein AL1, Kleinman HK.
[15] - J Orthop Res. 2014 Oct;32(10):1277-82. doi: 10.1002/jor.22686. Epub 2014 Jul 8. Thymosin ß4 administration enhances fracture healing in mice. Brady RD1, Grills BL, Schuijers JA, Ward AR, Tonkin BA, Walsh NC, McDonald SJ.
[16]-Neuropharmacology. 2014 Oct;85:408-16. doi: 10.1016/.neuropharm.2014.06.004. Epub 2014 Jun 14. Beneficial effects of thymosin B4 on spinal cord injury in the rat. Cheng P1, Kuang F1, Zhang H', Ju G2, Wang J?.
[17] A. Duzel et al., ' "Stable gastric pentadecapeptide BPC 157 in the treatment of colitis and ischemia and reperfusion in rats: New insights," World J. Gastroenterol., vol. 23, no. 48, pp. 8465-8488, Dec. 2017. [PubMed]
[18] M.-J. Hsieh et al., "Therapeutic potential of pro- angiogenic BPC157 is associated with VEGFR2 activation and up-regulation," J. Mol. Med. Berl. Ger., vol. 95, no. 3, pp. 323-333, 2017. [PubMed]
[19] Z. Grabarevic et al., "The influence of BPC 157 on nitric oxide agonist and antagonist induced lesions in broiler chicks," J. Physiol. Paris, vol. 91, no. 3-5, pp. 139-149, Oct. 1997. [PubMed]
[20] - Expert Opin Biol Ther. 2015;15 Suppl 1:5139-45.do:10.1517/14712598.2015. 1011617. Epub 2015 Jun 22. Advances in the basic and clinical applications of thymosin B4. Goldstein AL1, Kleinman HK.
[21] - Lymphokine Res. 1989 Winter;8(4):383-91. Modulation of thymosin alpha 1 and thymosin beta 4 levels and peripheral blood mononuclear cell subsets during experimental rhinovirus colds. Hsia J', Sztein MB, Naylor PH, Simon GL, Goldstein AL, Hayden FG.
GHK-CU References
[1] L. DO. Sever'yanova and M. E. Dolgintsev, "Effects of Tripeptide Gly-His-Lys in Pain-Induced Aggressive- Defensive Behavior in Rats," Bull. Exp. Biol. Med., vol. 164, no. 2, pp. 140-143, Dec. 2017. [Springer]
[2] L. DO. Sever'yanova and D. V. Plotnikov, "Binding of Glyprolines to L-Arginine Inverts Its Analgesic and Antiagressogenic Effects," Bull. Exp. Biol. Med., vol. 165, no. 5, pp. 621-624, Sep. 2018. [PubMed]
[3] X. Wang et al., "GHK-Cu-liposomes accelerate scald wound healing in mice by promoting cell proliferation and angiogenesis," Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc., vol. 25, no. 2, pp. 270- 278, 2017. [PubMed]
[4] L. Pickart, J. M. Vasquez-Soltero, and A. Margolina, "GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration," BioMed Res. Int., vol. 2015, p. 648108, 2015. [BioMed Research International]
[5] L. Pickart, J. M. Vasquez-Soltero, and A. Margolina, "The Effect of the Human Peptide GHK on Gene Expression Relevant to Nervous System Function and Cognitive Decline," Brain Sci., vol. 7, no. 2, Feb. 2017. [PubMed]
[6] H. Zhang, Y. Wang, and Z. He, "Glycine-Histidine-Lysine (GHK) Alleviates Neuronal Apoptosis Due to Intracerebral Hemorrhage via the miR-339-5p/VEGFA Pathway," Front. Neurosci., vol. 12, p. 644, 2018. [PubMed]
Nitrates
Glenn JM;Gray M;Wethington LN;Stone MS;Stewart RW;Moyen NE;, G. J. M. G. M. W. L. N. S. M. S. S. R. W. M. N. E. (2015). Acute citrulline malate supplementation improves upper- and lower-body submaximal weightlifting exercise performance in resistance-trained females. European journal of nutrition. https://pubmed.ncbi.nlm.nih.gov/26658899.
J;, W. B. K. A. N. W. K. S. (2015). Effects of supplemental citrulline malate ingestion during repeated bouts of lower-body exercise in advanced weightlifters. Journal of strength and conditioning research. https://pubmed.ncbi.nlm.nih.gov/25226311/.
W;, W. B. K. A. N. L. (2016). Effects of Supplemental Citrulline-Malate Ingestion on Blood Lactate, Cardiovascular Dynamics, and Resistance Exercise Performance in Trained Males. Journal of dietary supplements. https://pubmed.ncbi.nlm.nih.gov/25674699/.
Schwedhelm E;Maas R;Freese R;Jung D;Lukacs Z;Jambrecina A;Spickler W;Schulze F;Böger RH;, S. E. M. R. F. R. J. D. L. Z. J. A. S. W. S. F. B. R. H. (2008). Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: impact on nitric oxide metabolism. British journal of clinical pharmacology. https://pubmed.ncbi.nlm.nih.gov/17662090/.
M;, K. (1999). Nitric oxide metabolism and breakdown. Biochimica et biophysica acta. https://pubmed.ncbi.nlm.nih.gov/10320663/.
Coggan, A. R., & Peterson, L. R. (2018). Dietary Nitrate Enhances the Contractile Properties of Human Skeletal Muscle. Exercise and Sport Sciences Reviews. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6138552/.
Hernández A;Schiffer TA;Ivarsson N;Cheng AJ;Bruton JD;Lundberg JO;Weitzberg E;Westerblad H;, H. A. S. T. A. I. N. C. A. J. B. J. D. L. J. O. W. E. W. H. (2012). Dietary nitrate increases tetanic [Ca2+]i and contractile force in mouse fast-twitch muscle. The Journal of physiology. https://pubmed.ncbi.nlm.nih.gov/22687611/.
J. Bailey, S. (2011). The nitrate-nitrite-nitric oxide pathway: Its role in human exercise physiology20. Taylor & Francis. https://www.tandfonline.com/doi/abs/10.1080/17461391.2011.635705.
Jones, A. M. (2014, May). Dietary nitrate supplementation and exercise performance. Sports medicine (Auckland, N.Z.). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4008816/.
Coggan, A. R., Leibowitz, J. L., Kadkhodayan, A., Thomas, D. P., Ramamurthy, S., Spearie, C. A., Waller, S., Farmer, M., & Peterson, L. R. (2015, August 1). Effect of acute dietary nitrate intake on maximal knee extensor speed and power in healthy men and women. Nitric oxide : biology and chemistry. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4362985/.
Mosher SL;Sparks SA;Williams EL;Bentley DJ;Mc Naughton LR;, M. S. L. S. S. A. W. E. L. B. D. J. M. N. L. R. (2016). Ingestion of a Nitric Oxide Enhancing Supplement Improves Resistance Exercise Performance20. Journal of strength and conditioning research. https://pubmed.ncbi.nlm.nih.gov/27050244/.
Larsen FJ;Schiffer TA;Borniquel S;Sahlin K;Ekblom B;Lundberg JO;Weitzberg E;, L. F. J. S. T. A. B. S. S. K. E. B. L. J. O. W. E. (2011). Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell metabolism. https://pubmed.ncbi.nlm.nih.gov/21284982/.
Richards, J. C., Racine, M. L., Hearon, C. M., Kunkel, M., Luckasen, G. J., Larson, D. G., Allen, J. D., & Dinenno, F. A. (2018, January). Acute ingestion of dietary nitrate increases muscle blood flow via local vasodilation during handgrip exercise in young adults. Physiological reports. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5789727/.
Bailey SJ;Fulford J;Vanhatalo A;Winyard PG;Blackwell JR;DiMenna FJ;Wilkerson DP;Benjamin N;Jones AM;, B. S. J. F. J. V. A. W. P. G. B. J. R. D. M. F. J. W. D. P. B. N. J. A. M. (2010). Dietary nitrate supplementation enhances muscle contractile efficiency during knee-extensor exercise in humans. Journal of applied physiology (Bethesda, Md. : 1985). https://pubmed.ncbi.nlm.nih.gov/20466802/.
Whitfield, J., Ludzki, A., Heigenhauser, G. J. F., Senden, J. M. G., Verdijk, L. B., van Loon, L. J. C., Spriet, L. L., & Holloway, G. P. (2016, January 15). Beetroot juice supplementation reduces whole body oxygen consumption but does not improve indices of mitochondrial efficiency in human skeletal muscle. The Journal of physiology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4713742/.
Larsen FJ;Schiffer TA;Borniquel S;Sahlin K;Ekblom B;Lundberg JO;Weitzberg E;, L. F. J. S. T. A. B. S. S. K. E. B. L. J. O. W. E. (2011). Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell metabolism. https://pubmed.ncbi.nlm.nih.gov/21284982/.
GS;, C. P. T. G. S. J. Z. (2015). The effect of l-citrulline and watermelon juice supplementation on anaerobic and aerobic exercise performance. Journal of sports sciences. https://pubmed.ncbi.nlm.nih.gov/25517106/.
Gonzalez AM;Spitz RW;Ghigiarelli JJ;Sell KM;Mangine GT;, G. A. M. S. R. W. G. J. J. S. K. M. M. G. T. (2018). Acute Effect of Citrulline Malate Supplementation on Upper-Body Resistance Exercise Performance in Recreationally Resistance-Trained Men. Journal of strength and conditioning research. https://pubmed.ncbi.nlm.nih.gov/29210953/.
Hwang, P., Morales Marroquín, F. E., Gann, J., Andre, T., McKinley-Barnard, S., Kim, C., Morita, M., & Willoughby, D. S. (2018, June 27). Eight weeks of resistance training in conjunction with glutathione and L-Citrulline supplementation increases lean mass and has no adverse effects on blood clinical safety markers in resistance-trained males. Journal of the International Society of Sports Nutrition. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6020314/.
Campbell B;Roberts M;Kerksick C;Wilborn C;Marcello B;Taylor L;Nassar E;Leutholtz B;Bowden R;Rasmussen C;Greenwood M;Kreider R;, C. B. R. M. K. C. W. C. M. B. T. L. N. E. L. B. B. R. R. C. G. M. K. R. (2006). Pharmacokinetics, safety, and effects on exercise performance of L-arginine alpha-ketoglutarate in trained adult men. Nutrition (Burbank, Los Angeles County, Calif.). https://pubmed.ncbi.nlm.nih.gov/16928472/.
JE;, L. J. R. U. R. A. (2012). Nitric oxide and voluntary exercise together promote quadriceps hypertrophy and increase vascular density in female 18-mo-old mice. American journal of physiology. Cell physiology. https://pubmed.ncbi.nlm.nih.gov/22322971/.
Schoenfeld, B. (2010). The mechanisms of muscle hypertrophy and their application to resistance training. Journal of strength and conditioning research. https://pubmed.ncbi.nlm.nih.gov/20847704/.
Cholewa, J., Trexler, E., Lima-Soares, F., Pessôa, K. de A., Sousa-Silva, R., Santos, A. M., Zhi, X., Nicastro, H., Cabido, C. E. T., Freitas, M. C. de, Rossi, F., & Zanchi, N. E. (2018, October 10). Effects of dietary sports supplements on metabolite accumulation, vasodilation and cellular swelling in relation to muscle hypertrophy: A focus on "secondary" physiological determinants. Nutrition. https://www.sciencedirect.com/science/article/abs/pii/S0899900718303939.
Neale A Tillin 1, Sarah Moudy, Kirsty M Nourse, Christopher J Tyler, N. A. T. 1, S. M. K. M. N. C. J. T. (2018). Nitrate Supplement Benefits Contractile Forces in Fatigued but Not Unfatigued Muscle. Medicine and science in sports and exercise. https://pubmed.ncbi.nlm.nih.gov/29727405/.
Husmann, F., Bruhn, S., Mittlmeier, T., Zschorlich, V., & Behrens, M. (2019, March 22). Dietary Nitrate Supplementation Improves Exercise Tolerance by Reducing Muscle Fatigue and Perceptual Responses. Frontiers. https://www.frontiersin.org/articles/10.3389/fphys.2019.00404/full.
Lactate Research Citations
Nalbandian, M., & Takeda, M. (2016, October 8). Lactate as a Signaling Molecule That Regulates Exercise-Induced Adaptations. Biology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5192418/.
Rabinowitz, J. D., & Enerbäck, S. (2020, July 20). Lactate: the ugly duckling of energy metabolism. Nature News. https://www.nature.com/articles/s42255-020-0243-4.
Brooks, G. A. (2018). The Science and Translation of Lactate Shuttle Theory. Cell Metabolism, 27(4), 757–785. https://doi.org/10.1016/j.cmet.2018.03.008
Brooks, G. A. (2009, November 30). Cell–cell and intracellular lactate shuttles. The Physiological Society. https://physoc.onlinelibrary.wiley.com/doi/full/10.1113/jphysiol.2009.178350.
Brooks, G. A. (1985). Lactate:Glycolytic End Product and Oxidative Substrate During Sustained Exercise in Mammals — The “Lactate Shuttle.” Proceedings in Life Sciences, 208–218. https://doi.org/10.1007/978-3-642-70610-3_15
Brooks, G. A. (2002, April 1). Lactate shuttles in Nature. Portland Press. https://portlandpress.com/biochemsoctrans/article-abstract/30/2/258/63601/Lactate-shuttles-in-Nature?redirectedFrom=fulltext.